The art of long labor involves helping a mother keep up her morale while addressing her body’s needs for marathon activity. We can help soothe the mother by helping her ease her busy mind or labor pain when possible.
Long labors can be a result of the cultural misunderstanding of human physiology. It’s true that women are designed for birth, but modern life isn’t exactly designed for women. Hours sitting at desks and behind the wheel, for example, are postural restrictions that were not in the design plans for sacro-ischial joints or the psoas erectors.
When the issue is in the tissue there is something we can do. Tight muscles and tight ligaments can be relaxed with bodywork and things the mother can do either by herself or with help.
With trust, patience, and a bit of a balancing act, a woman experiencing long labor can possibly overcome the effects of hours of sitting or standing and achieve tangible labor progress.
“Wait! Can I do something before birth so I have an easier birth (than if I didn’t prepare with the Spinning Babies® approach?”
Why, yes, we also have things to watch and do in pregnancy for parents at our Shop.
A long early labor concerns many women. It takes a lot of attention and mental energy, and it’s easy to wonder if the next contraction will be the one to really do something.
This is the time when a lot of questions flood into your head. When should you call the doula or doctor? When will your partner come home? What should you do about the other children? When does the pain start? With all of this on your mind, you can easily tire yourself out before labor even really begins.
During this stage, it’s very important to eat. Eating foods that are easy to digest, like simple soups, smoothies, or yogurt are a few great options. Toast is a classic, but not too nutritious, so don’t forget root vegetables and an easy-to-digest protein. I craved a salmon sandwich and enjoyed salmon for the first time in my life during the early part of my second labor.
Outside factors may be at play. Long early labor might occur for a woman who has had a few babies already. Sensitivity to estrogen surges can bring on nighttime Braxton-Hicks or practice contractions (a friend calls these “squeezies”). A full moon or approaching weather front (barometric pressure drop) can bring on practice contractions or cause a gradual, slow beginning as well.
Try to get some rest. If you can rest normally (i.e. getting good sleep at some point in each 24-hour period), things are generally going to be fine. Don’t forget to keep in touch with your birth attendants and relax as best you can.
The length of labor is a separate issue than the pain of labor. A long labor with unexpected strength and little to no progress is called a stall in labor. It’s technically only a stall if it’s after 4 cm, though we want to pay attention to why labor stopped if it’s before 4 cm too, especially if your water has already broken.
Some women just need time in labor. How do we know whether a laboring woman experiencing challenges needs techniques or a little more time? Oftentimes the waiting gets done in a hurry and quickly turns into, “I’ve had it, give me the epidural now!” If the mother doesn’t want to do techniques, that’s fine—don’t push her. But if she needs some encouragement, try a little love and support!
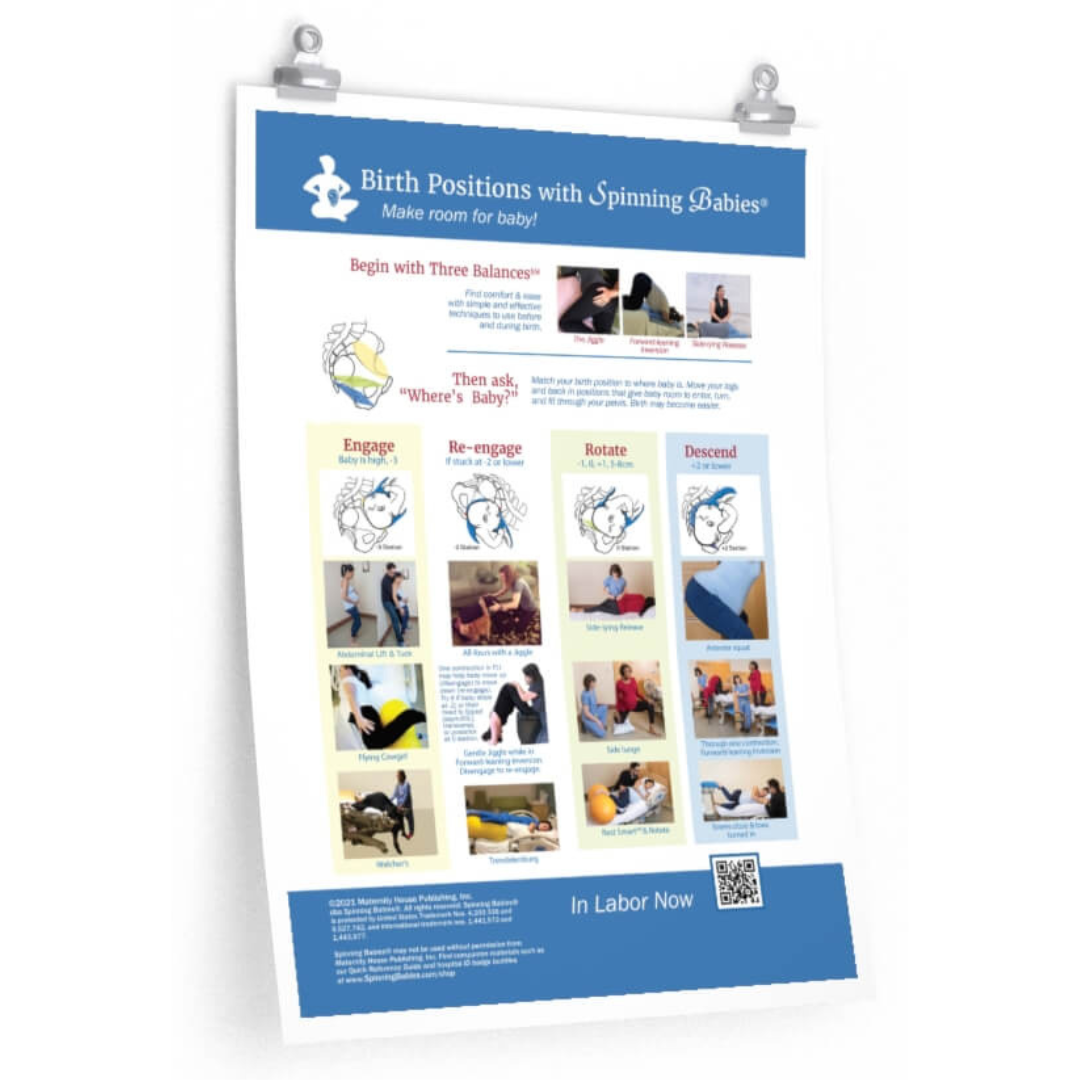
In labor, there is a series of four techniques that solve most stalls, especially in the presence of contractions:
If no contractions: Get some sleep (without drugs if you can) and eat some oatmeal or other healthy carbs to restore a labor pattern. Follow these up with rest in a Rest Smart℠ position.
The techniques to overcome a labor stall differ a little if you are in bed or if you are able to be up and moving. If you can get up, try standing with your knees soft (not locked) and lean over a friend or a counter-top, etc. If you are in bed due to sickness, high blood pressure, or an epidural, use the Roll-Over positions as best you can.
At this point, the mother may feel that her labor is going again. Contractions may be strong and close, or mild and close together—but then they slow down altogether. Then, later, they start up again.
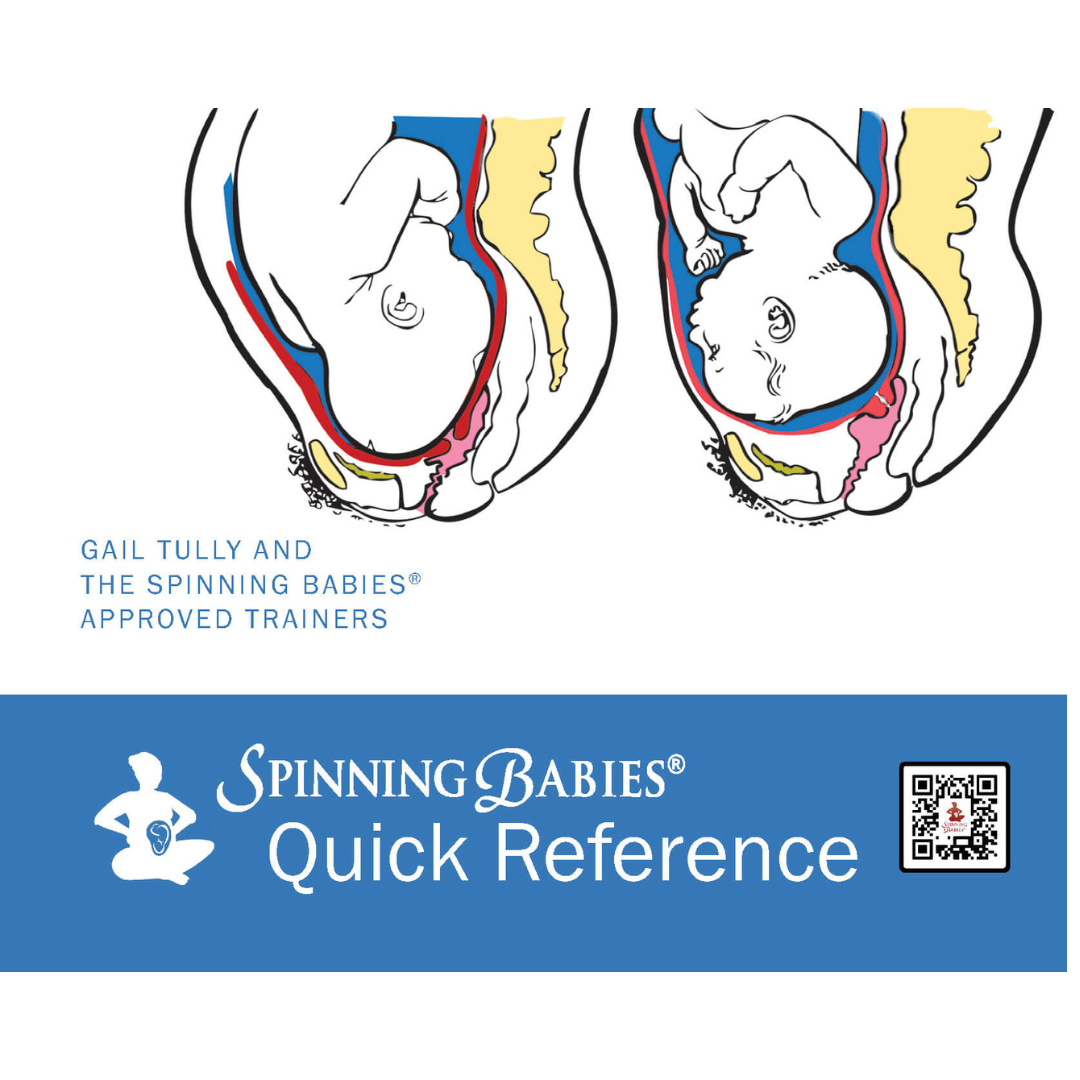
Is it labor or is it only a promise? It hurts, so it must be labor. But the cervix isn’t opening, so it can’t be labor. Which is it? The mother’s body may be ready, but sometimes with a posterior baby, the baby just isn’t fitting into the pelvic brim. We need to help the baby tuck the chin and rotate.
Is the baby in an ideal or anterior position? Then it’s time to get the chin tucked. If your contractions have stopped or are mild for now, you should rest and then eat while you wait for the contractions to return. Once the baby is engaged, the uterus may require a rest. As long as mom and baby have no clinical signs of trouble or fetal distress, a good nap is just the thing to protect the labor later. After a good snore, eat a bowl of oatmeal. The uterus will pick up again once you’re rested and fed. If the baby has rotated and/or engaged, labor will start again.
Back labor may be the result of tight ligaments, tight or weak muscles, or the baby’s position. Low-waisted women are more likely to go through back labor, as the baby is often longer than the mother’s torso.
There is a simple technique that works wonders for back labor. When you can anticipate a contraction coming (contractions have to be somewhat regular), begin an Abdominal (Belly) Lift and hold it during the contraction. Let go of your belly in between contractions, then repeat ten times as described. This will shift the force of the uterine action (contraction) from your back to your cervix and angle the baby better. With success, the cervix will begin to dilate.
For the next several contractions, stand with soft knees and lean forward. Let there be a little movement in your knees to help you be more intuitive with your body signals and allow your pelvis to move better. Leaning forward encourages babies to rotate and labor to progress. If your belly hangs over your pubic bone, try wearing a pregnancy belt to help.
A first-time mother can expect her active labor phase (the part of labor that opens her cervix from 4 cm to 10 cm dilation) to last from 12 to 24 hours. If labor is shorter, that’s great, but it’s not helpful to assume that labor will be short because her mother’s labor was short or because she has a great attitude (although those are both certainly good things).
Eat and sleep during any lull period. Again, we want to protect the health of the mother and baby with food and rest for the journey. She doesn’t have to be constantly reminded to eat and drink, but watching the clock discretely and making sure she’s eating at least a 1/2 cup of food or so every couple of hours is a minimum once she’s passed 6-8 hours of labor.
Emptying the bladder is important, too. If the baby remains high, ask the nurse or midwife (if she isn’t already) to monitor how much urine is actually coming out.
If the cervix is fully dilated and the mother doesn’t have an urge to push, suggest a Rest Smart℠ position and let her sleep. When she wakes, make sure she eats something.
Provide emotional support. Emotional support during the second stage can help a woman trust the downward pressure sensations and reduce resistance to let the baby descend and come past the rectum and onto the perineum. These can be overwhelming sensations, so a little reassurance and a practical attitude are helpful.
Let the urge come on and teach the mother through natural body sensations when and how to push. If necessary, change positions to encourage the urge and the opening of the pelvis. Opening and moving the pelvic joints is helpful during a contraction.
Good breathing habits are more important than time. Holding the breath frequently can be harmful after a while. When the baby is getting a good oxygen exchange between contractions, this helps the baby’s overall stamina.
An experienced midwife or physician can help a woman through a long second stage. I’ve heard of 24-hour second stages with active pushing times of 5-8 hours with great outcomes. But listening to the baby is more important than the time it takes. A long second stage requires skilled help from an experienced assistant.
Offer food and rest again. Nutrition is almost always easier during the second stage than the first (dilation). Resting is also an option. Changing positions frequently is a smart thing to do too. Basically, if what you’re doing isn’t working, try something different!
Too often a swollen cervix sends birthing women to the operating room. The cervix opens like an oval ring, getting wider and more round as the baby’s head presses down during fetal descent in labor. Effacement of the cervix is when the cervix gets thinner, which helps the cervix to open. Because we expect the cervix to get thinner, it can be alarming when the cervix stops opening and swells.
This doesn’t mean that the baby won’t be able to fit once he or she (often with a little help) can find their way through the lower pelvis. The uterus will continue to contract, as it tries to correct the baby’s position.
The baby may or may not be able to fix this spontaneously. Time without helping the baby to fit may only stress the womb or baby. But when we understand the need, we can begin to address the issue more intelligently. Necessary changes include flexion, rotation to a better position, and/or molding better to fit.
Swollen cervixes will recede when the baby’s head shifts and allows circulation. We can also move the mother to improve circulation. The cause of the stall with swelling is often a need for further flexion and rotation for the baby to line up with the lower portions of the pelvis.
But we cannot forget fear or disturbance of the birthing environment as a causative factor. It’s important to understand the signs of labor in which the baby can’t fit and to see the difference between a stall in labor and signs that the baby is really too big for the mother’s pelvis.
The premature urge to push can be a real annoyance. Pushing on a cervix that isn’t ready may tear it, although that’s rare. Pushing early sometimes causes cervical swelling as well.
I believe it is uterosacral ligament tension that causes the early urge to push. There may be deflexion (chin up) or occiput posterior presentation with that tight or twisted ligament as well.