How do you know whether your labor will be easy or hard?
Birthing is experienced across a wide spectrum of possibilities.
Unusual ease or challenge are uncommon experiences.

Many first births may involve more physical work than expected. That’s why we call it “labor.” The work involved in opening to birth can be a beautiful expression of one’s own life.
Spinning Babies® offers an approach to help more parents experience childbirth towards the easier side of the spectrum of possibilities. Let’s take a look at the spectrum and where you might find yourself on it.
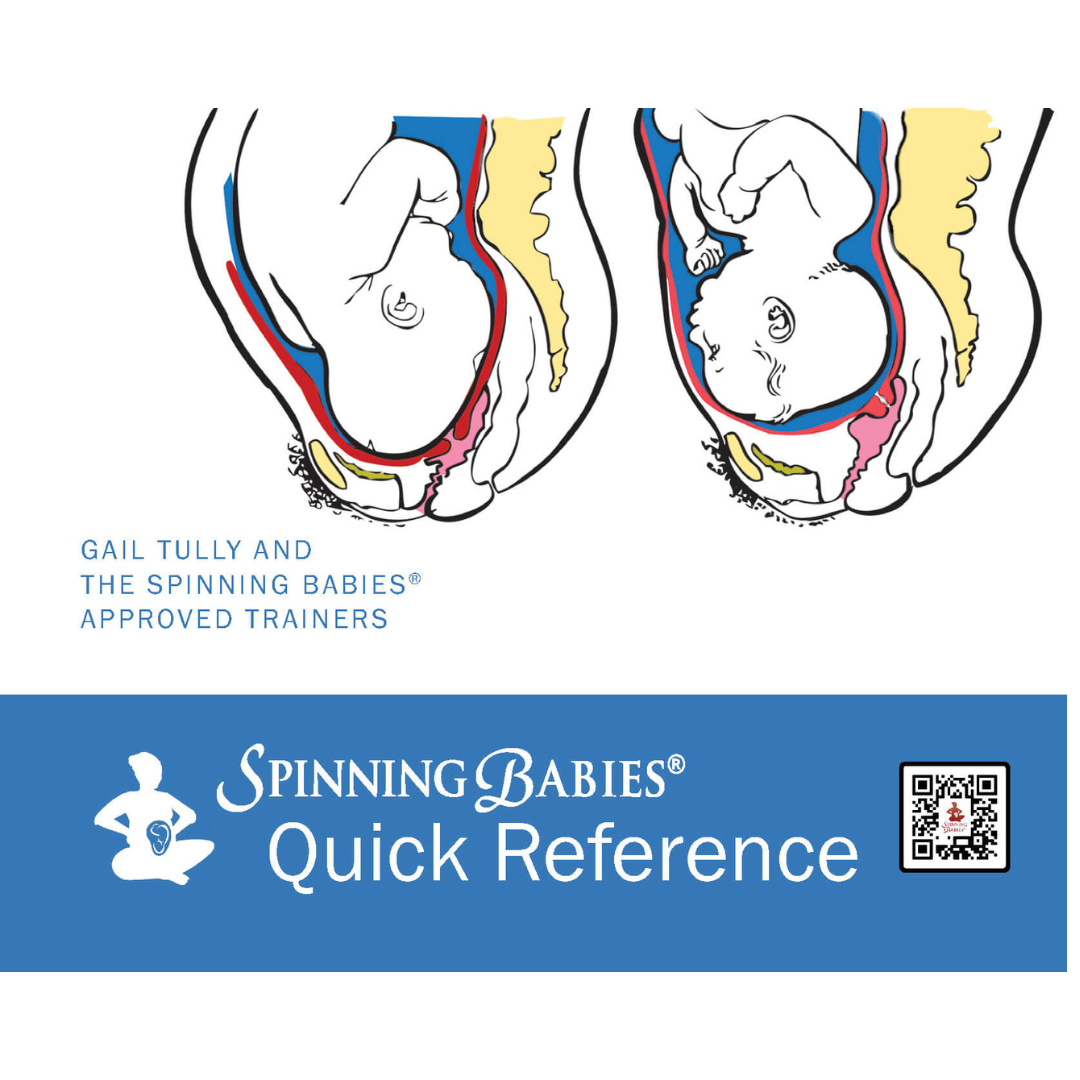
For instance, research shows a posterior labor (baby faces the front, spine-to-spine) may be longer and need more professional help than a labor with a baby in the anterior position (facing the back, spine toward the abdomen or left). it’s unusual to have a super-easy posterior. While sometimes a cesarean is needed for a posterior baby, most posterior babies rotate in labor.
One reason for a cesarean to finish a posterior labor is baby doesn’t fit. But seriously, too many women are given cesareans because no one there knew what to do to help the baby rotate so the baby could fit!
Balance moves you toward the easier side of the spectrum. When the muscles are in balance, then it’s up to the bones when a baby is in a good position.
There is a spectrum of how hard and painful any labor might be, and that includes labor with the baby in a posterior presentation. I believe ease has more to do with the symmetry of the muscle tensions in the body and the angle of the pelvis in a mis-chosen birth position than the size of the pelvis or even the baby’s position
A malposition is when baby can’t fit due to their position in the pelvis without causing a dangerous level of exhaustion or harm. Nature wouldn’t make that fetal position normal. Such a malposition is usually a symptom of asymmetry or another imbalance, but could sometimes be caused by how an arm is positioned, or the cord or placenta makes a position improvement unavailable.
Balancing activities that keep the pelvic joints gently and regularly mobile will make any labor easier than it would have been with an imbalance or stiffness.
Choosing a caregiver who understands both physiological birth and how to use interventions only as needed can make the difference between vaginal birth and finishing with major surgery. Supportive birth helpers speak to the body, the heart, and the mind.
How your caregiver attends to and manages your labor will also affect your experience. Some providers want to do something early while others have a wait-and-see approach. Which is right?
“Clear evidence shows midwifery care, “community birth” settings (birth center and home birth settings), and doula support(including the extended model of prenatal, childbirth, and postpartum support) provide excellent and appreciated woman- and family-centered experiences, leading to improved birth outcomes.” -National Partnership
Many pregnant parents with a natural birth plan are seeking care from an obstetrician. While I know a few obstetricians who trust the birth process and are patient to wait during long labor with a healthy mother and baby, many just don’t have the exposure to spontaneous, natural birthing.
When labor is long or painful, drugs are often offered to dampen or hurry the experience, or surgical tools to shorten or finish the birth. Unless interventions are needed to avoid suffering, dangerous risks, or death, physiological birth practices should be the first choice to help reduce pain or the time of labor. After adding body balancing, emotional support, and better birth positioning, then either the baby may be born or the necessary intervention may be easier on baby. Working with a doctor or midwife will improve the determination whether time is available to use a body-centered technique before a surgical one.
Seeking help outside the medical system (a home birth midwife or doctor) is another way a woman might achieve her natural birth plan.
Adding a doula to the hospital birth experience reduces the amount of pain a woman perceives (statistically according to surveys) and has been shown to shorten active labor. A trusted doula moves your birth toward the easier side of the birth spectrum. Some doulas are also helpful at a home birth situation and perhaps they had a home birth themselves. Doulas have been proven to improve birth outcomes in randomized control studies.
Having a history of one or more of the following conditions could mean that your body is storing some of that stress in the form of tightened muscles. It may not be obvious either, as you may feel no discomfort now if an event happened long ago or came on gradually.
Remember, I am addressing a variety of causal factors. People are too complex to share the same results from the same events. Knowing your history can help set your expectations to better match your unique experience.
Your baby’s positioning is a significant factor when it comes to the ease of a labor. This is something you can—and should—be keeping track of.
Belly Mapping℠ is a method I’ve developed to help you make a picture of the fetal position using the the baby’s kicks and wiggles inside the womb. Give it a try today!