The pain may be on the pubic bone, or felt in the middle of the back, the outer tips of the hips or, rarely, rectum. But the abdomen is less likely to be the location of where the contractions are felt.
When baby moves, baby may “grind” their forehead on the pubic bone in an attempt to rotate away from the front of the pelvis.
Sometimes there isn’t pain to give a clue, as the cervix is often open less than 3 cm in a first-time mom. Don’t rely on cervical dilation to verify where baby is, though! Sometimes the cervix will open all the way to 10 cm and the baby hasn’t even come into the pelvis yet.
If the baby isn’t engaged, the nurse, midwife, or doctor may say the baby is -3 station. This unengaged posterior baby often must rotate into left occiput transverse before engaging. Spinning Babies® techniques aim to help in this rotation. Rotation may solve this problem and let baby engage and descend through the pelvis, helping the birthing person potentially avoid a cesarean.
The mother can check her own abdomen for a little tell-tale “ledge” resting on her pubic bone. If the ledge is there, it’s typically baby’s forehead. Now we know contractions may start and stop until the baby is turned.
When baby is directly posterior, the back of the head might be felt in the pelvis and the provider often thinks the baby is engaged. This may also be because the head won’t wiggle. If the forehead overlaps the pubic bone, then the forehead isn’t in the pelvis and the baby isn’t truly engaged.
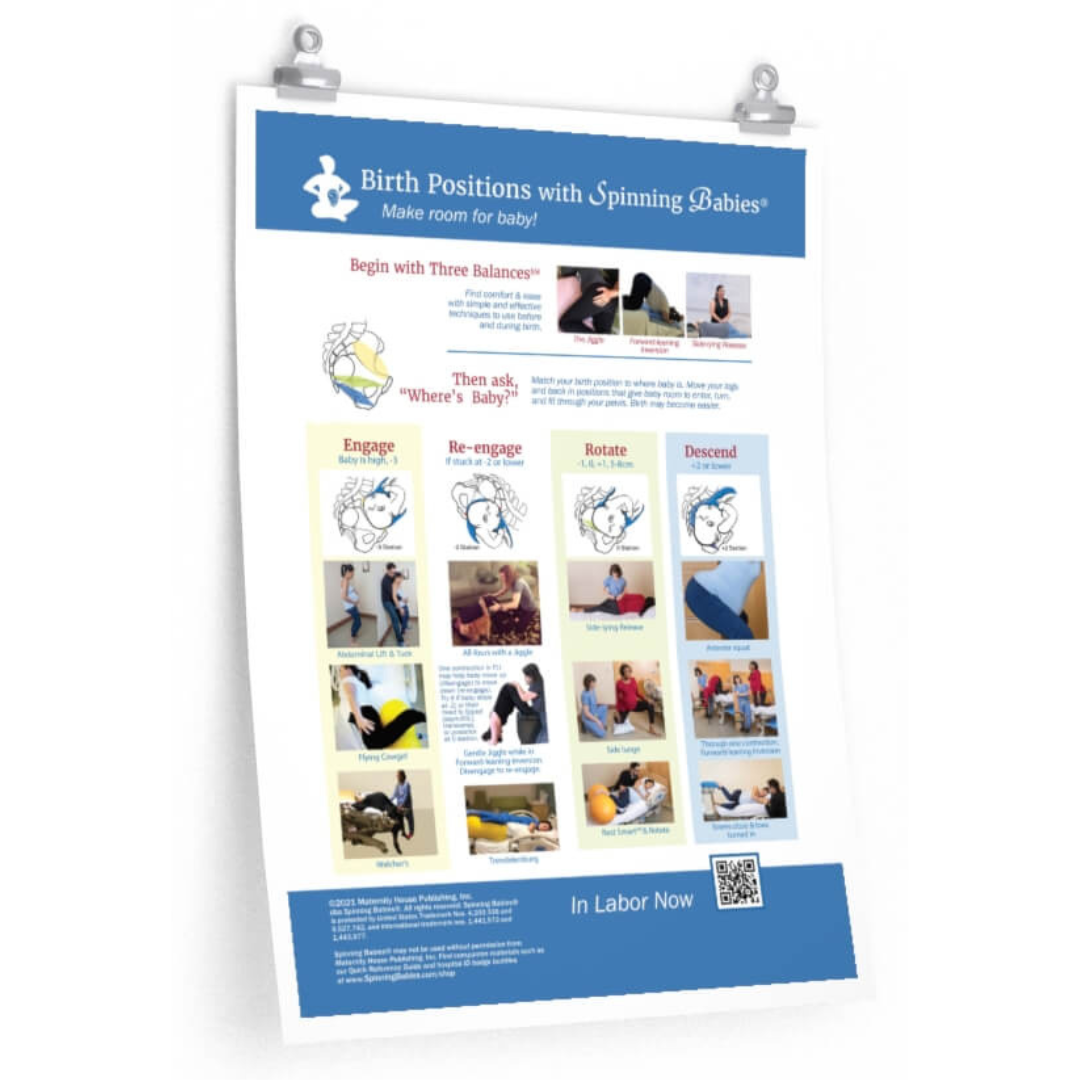
For many women in this situation, the Three Balances℠ relaxes the mother’s abdomen and makes room for fetal rotation.
Now the laboring woman can often rest, as the labor may be mild for an hour or so. She can snooze until surges begin again. If a woman isn’t pushing her baby out, she should follow the Three Balances℠ with the techniques to match the pelvic level.
Is the baby still too high? We already balanced, so now we need to reposition the baby for flexion. Do the Abdominal Lift and Tuck through a contraction for 10 contractions in a row. Let the belly down and relax the back in between contractions. Doing the Abdominal Lift with a posterior pelvic tilt will flatten the lower back and move the sacral promontory out of the way, which will help baby to tuck the chin and rotate out of posterior and descend.
If not, baby is now in either zero (“0”) station in the mid-pelvis, +1 station, +2 station, or lower down in the outlet. Either way, strong efforts aren’t progressing the labor. Do 3 lunges on each leg, resting between contractions. This series of techniques will help the vast majority of people.
You may need help with more techniques to turn a posterior baby, including a manual rotation of the baby by her OB or Midwife (done internally). If the posterior baby is too large for the mother’s pelvis and the mother’s ligaments are tight, an excellent fascial therapist who is specially trained in pregnancy may be necessary to avoid a cesarean. To prevent that crisis in a labor, begin this process early on in the pregnancy to release spasms and imbalance in the body (specifically the pelvis) to promote optimal fetal positioning in labor.
These Balances work to balance the pelvis in pregnancy and in labor. Starting your balance early on in the pregnancy may mean you won’t need them during labor and you don’t end up with a crisis due to a stalled labor or a case of “baby won’t fit.”
Sometimes Baby’s head is deep in the pelvis but doesn’t keep going down. Tight muscles or a lack of room might be the reason.
The head is engaged. The head is on the cervix now. Perhaps the cervix is 4 or 5 cm dilated or more.
You feel pressure on the sides of the insides of your hips. The pelvic floor may feel a sharp ache with contractions. There may be a bit of panic or fear.
What to do now?
The Side-lying Release can be the fast way to sigh in relief. Three contractions on each side between and during contractions is recommended but two may be adequate. This can be repeated if taking a short cut was actually a longer detour.
After Side-lying Release find a way to rest with the hips tipped a bit. This is called asymmetrical hips. A lunge to the side is the most obvious example. You can lie on your side in bed and put your upper leg up and over a peanut ball or a pile of pillows. You can half deflate a round birth ball to make it behave like a peanut ball. Sitting on the toilet for three contractions with one foot on a stool and the other foot on the floor is another way to create asymmetry in your hips. This gives baby more space. After three contractions with one foot lifted, switch the feet and legs around.
Or we almost do. Baby is low and the body is suddenly bearing down on its own. Or, you are being told to push.
Fear of pushing is a social thing. You might poo, you might tear. It’s not a lovely picture. So, turn off the light, if you think like that.
Believe me, your midwife will see poo-ing as a good sign. You never see anyone happier about poo except new parents admiring the plumbing of their new baby!
The urge to push builds slowly or comes suddenly and both are just as normal. If baby is coming fast, lay down so baby doesn’t fall on the floor or into the toilet. If baby is coming slow, change positions after 3 contractions to find the one that gives space for baby to come down a bit easier.
You may have caught the clue that the pressure of a poo is part of the second stage of labor/labour. This sensation comes with the peak of a contraction. As baby comes lower, you’ll feel your bones actually moving apart. This may give you guidance in how to arrange your legs and back to help baby fit. Trust your body and neither shut it down nor blast your baby out with a super-charged push. Your skin will thank you.
As baby comes low into your pelvis, putting your knees together but only with your heels wide apart gives space. Turn your toes in to twist your thigh and widen your sitz bones. This is called internal rotation of the femur (thigh bone). Now baby has an inch more room between the sitz bones (ischial tuberosities).
You can push hard before you feel your skin stretching and burning. At that point in pushing, back off and let your skin have a moment. After three contractions of passive pushing, if baby is moving down spontaneously you can go back to directed or forcefully pushing until you feel the “ring of fire” or stretch of the perineum.
At that point, pant. Once the baby is down on the perineum, you can ease up and see, once again, if baby moves lower with lighter pushing.
If baby’s head is angled in a posterior position, you may have to push hard throughout to get baby moving. Then it’s really important to make room between your bones with smarter birth positions.
The most important baby position is on your chest next to your heart in the hours and days after birth. Skin-to-skin is best for brain and heart coherence together (with a diaper if you want to catch the tarry meconium poo that comes the first couple days).
If separation occurs, recreate the moment with skin-to-skin in a dark room with the baby. Make the moment sensitive, quiet and restorative. You deserve it! Your brain will awaken certain parenting intelligences when you nurture your self and your baby this way. It’s not that you don’t have other advantages. But why not drink water when your thirsty, sleep when you’re tired, and greet your baby as nature intended when you come to the moment of holding your baby the first time?