A classic here at Spinning Babies®, the Forward-Leaning Inversion (FLI) optimizes room in the lower uterus for baby to get into a more ideal position for birth. Helps:
A classic here at Spinning Babies®, the Forward-Leaning Inversion (FLI) optimizes room in the lower uterus for baby to get into a more ideal position for birth. Helps:
The Forward-Leaning Inversion technique comes from Dr. Carol Phillips, DC of Dynamic Body Balancing.
The Forward-Leaning Inversion (FLI) lets the uterus hang by its own ligaments to slightly lengthen, thereby untwisting the ligaments supporting the lower uterus and cervix.
The cervix may become less tipped or tight and then be able to let the baby’s head position better. We believe this technique prepares the cervix to dilate in labor more easily.
Reduce back, hip, or tailbone pain with repeated Forward-Leaning Inversion (FLI) (once daily is usual). Improved fetal positioning may result. A breech or transverse baby may turn head down. Forward-Leaning Inversion (FLI) can be done even if baby is head down and there are no suspected positioning issues.
Please be careful when attempting this technique. Don’t drop into place. Move slowly and be controlled to prevent falls and protect your placenta and ligaments from a jolt.

Learn how to do the Forward-Leaning Inversion by reading the directions below out loud with your helper. You can also watch it taught on video in our Birth Preparation online course or in our Spinning Babies® Parent Class and Daily Essentials videos. Parents across the globe are using these techniques for comfort in pregnancy and easier birth—and they’re working! Both are available on digital download/streaming.
You need a stable surface to kneel on higher than the spot where your elbows will rest.
Before you start, do some shoulder and neck circles to warm up.

Do a Forward-leaning Inversion once daily for 30 seconds (roughly three breaths).
Breech or Sideways? After 30 weeks of gestation, we have some more tips. See our pages on breech or transverse (lying sideways) baby positions for additional recommendations.
Please note: Our body warns us with a throbbing head when we first get upside-down. After 3-6 times, your body will realize you intend to be upside-down, and your head will stop pounding. Just get up early if this happens and try again, one time each day. The feeling will go away soon enough.
You may like to do a Forward-leaning Inversion once in early labor just to ease cervical dilation (shorten labor or lessen labor pain). That would be a proactive use of FLI.
Sometimes, labors take longer than expected. Sometimes, labor hurts more than it is easy to cope with the pain. Perhaps there are strong contractions without progress in cervical dilation. Sometimes, a baby might be found to be in a less-than-ideal position, with the back on the right or towards your baby (spine-to-spine). Or sometimes baby is waiting behind a bone. Please consider doing a Forward-leaning Inversion in any of these situations. If you can hold the position for one contraction, then the contraction will have another option to move the baby out of the stuck position, or the pain may be less afterward, too.
This technique is also particularly helpful for a tight or swollen cervix, asynclitism (add Side-lying Release), deep transverse arrest (add Side-lying Release), or when a baby simply won’t come down despite a good position (add psoas release).
Remember: Don’t go fast; do your best to protect yourself from falling.

Coming back up to kneeling makes this technique work best!
In a hospital bed,
If you are not in a hospital bed, simply follow the instructions in the pregnancy description above. Remember to:
Use a stool or step if you’d like, to help you walk your hands down.
You can repeat the FLI through one more contraction (right away or about 15 minutes later).
Repeat FLI once during each phase of labor (early, active, and pushing) if necessary, but be sure to have a provider ready to catch the baby if you were pushing, just in case this was the technique you needed! You can do a FLI through more than one contraction, coming up between, when overcoming labor dystocia (stuck baby).
See this and other breech-turning techniques in Flip A Breech, or buy our Helping Your Breech Baby Turn ebook. If you like detailed instructions with video, See our Breech for Pregnant Parents online offering.
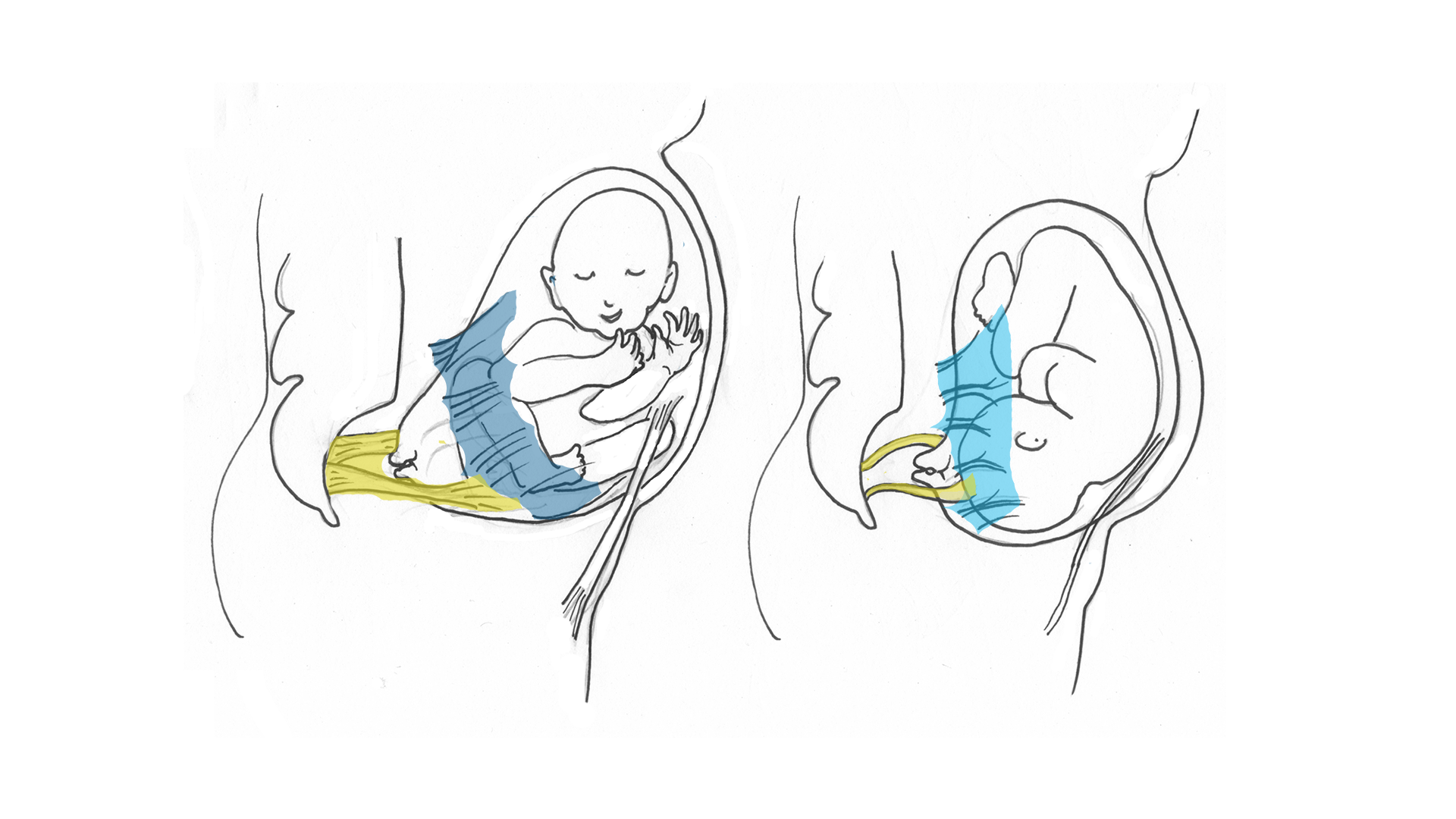
Tight before and loose after daily use of the Forward-leaning Inversion. These images don’t show a twist, but that can happen too.
All pregnant women without a contraindication can do the Forward-leaning Inversion:
Listen to your body and check out unusual symptoms with your physician BEFORE going upside down. Thousands of women are getting mild or dramatic benefits from the inversion, but there are risks. Here’s what we know at this time.
Round ligament pain happens occasionally with an inversion. Round ligament pain is not typical, nor health-threatening. Round ligament spasms can be resolved with the Webster, self-care, warmth, or a specific sort of self-massage. It’s okay to repeat the inversion carefully (for 30 seconds) even though this is happening. The inversions may resolve the spasm but the Webster is specific to resolving this type of ligament spasm.
A pain that persists more than a few minutes or is especially severe deserves attention. Report any abdominal or shoulder pain to your provider. Be sure you understand the warning signs in pregnancy.
Don’t drop fast! One mother whose abdominal muscles were very separated dropped fast from a high bed and partially separated the placenta. She and the baby had to remain under observation in the hospital until she gave birth several days later (the mother and baby were both healthy). Another woman with a history of placental issue and high blood pressure experienced separation and had to have an urgent cesarean.
 Please note: The cloth is NOT in the groin but rather on the thighs, helping hold the mother’s weight. If done during a labor contraction, a doula or calm loved one would be in front of her face and under the table to give eye contact.
Please note: The cloth is NOT in the groin but rather on the thighs, helping hold the mother’s weight. If done during a labor contraction, a doula or calm loved one would be in front of her face and under the table to give eye contact.
Emily and Ludvig are 36 weeks pregnant (8 months), and their baby has turned sideways — into a transverse lie.
Emily uses the inversion to help “balance” her cervical ligaments, which may be tight and twisting her lower uterus. She is also seeing a chiropractor and a midwife. If this doesn’t work, she may also visit a craniosacral therapist or Maya massage therapist. She’d like to have a natural birth, so it is important that the baby turn head down. The next day, the ultrasound done before the doctor tried to turn the baby showed the baby had turned head down!

We do see a couple actions that we have corrected in our education. Do come up to a high kneeling position and do so with someone holding on to your arm so you don’t fall if your blood volume can’t keep up with your movement upwards! Some people get light headed when they stand up, and so people can get light headed when they swing up to kneeling after FLI. Also, Emily puts one knee down before the other and this twists her symphysis pubis (pubic bone cartilage). That can strain the pubic bone and cause pain. Keep the knees together if you have to slide your knees off the couch or see how to do the mermaid when you get up. Here’s a photo of a good support hold for coming up to a high kneeling position after FLI – this is the best finish position before “mermaiding” your legs off the couch or bench.

After doing Forward-leaning Inversions for a week, you’ll likely notice more ease in your back and neck. Your shoulders will be stronger. You may feel more fit in general.
If baby has been head down, you may just feel more comfortable. Baby may not move to the left until labor, but this technique is helpful with other techniques to prepare the body so that baby can turn through the pelvis with more ease in labor.
A breech baby often needs more techniques than just FLI. However, when a breech baby turns head down, kicks will be stronger in the top of the uterus than they felt before. You may feel more of the baby’s weight in your pelvis, which may change the way you walk if you are late in pregnancy.
A baby in a transverse lie is lying sideways and in the last trimester of pregnancy, the pregnant belly generally looks wider side-to-side than top-to-bottom. When the baby moves into a vertical position, the womb will look different, suddenly becoming longer top to bottom and narrower on the sides.
Once head down, baby’s kicks will be strongest above the navel towards the ribs. One side of the womb may have a large portion of baby (the firm back) while the other side may feel softer and limbs might be felt. Alternatively, there may be limbs on both sides and “all over” the front without such an obvious firm side when baby faces the front. Learn more at Belly Mapping.
If you use this technique in labor, you’ll generally feel different afterward. There may be more comfort during contractions after the inversion (and sometimes during!). A baby is occasionally born quickly after an FLI aligns the uterus and baby if they were only a little off before. We see this sometimes when an FLI is done hours or days into a long labor. We notice that Daily Activities (or Daily Essentials) can sometimes prevent long labor or overwhelming labor pain.
If you have an inversion board, you can use that instead. Standing sacral release and chiropractic/osteopathic care are helpful too, although they won’t reach the uterosacral ligaments. Here is a blog about alternatives to FLI.
I’m not here to conflict with your provider’s advice. Here’s an email to show how providers sometimes think about FLI:
I was hoping you could help me out… a CNM who saw one of my clients told her not to do inversions because it could cause the baby to become breech. Any help that you could offer would be greatly appreciated!
My response was that the CNM had palpated this mother’s abdomen. Perhaps the mother has polyhydramnios (far too much amniotic fluid), or very loose muscle tone even with normal amniotic fluid. I add that Intrauterine Growth Restriction (IUGR), a condition caused by placental insufficiency, may be a reason not to do Forward-leaning Inversion.
A normal pregnant woman with a head-down baby who does the Forward-leaning Inversion for 30 seconds at a time is not likely to flip her baby to breech. Sometimes, a concern means the provider will advise to avoid an inversion. I’m going to leave the decision-making between the care provider and, perhaps, her experienced myofascial worker/chiropractor.
A provider might confuse Forward-leaning Inversion with the breech tilt or the Open-knee Chest position. These are not the same inversions, as they are done much longer. I’ve been recommending FLI for years and following many women through their pregnancies using this technique successfully. It is possible that a baby could turn breech.
Of the hundreds or possibly thousands of women doing this inversion, there are understandably going to be some bad outcomes. I would very much like to be told about these cases.
Report any complications of pain or immediate bleeding, and describe the situation exactly, including the date, gestational age, health concerns, the way you did the inversion, whether it was your first attempt or not, and the time of complication. You can email me at gail@spinningbabies.com.
Of the hundreds or possibly thousands of women doing this inversion, there are understandably going to be some bad outcomes. I would very much like to be told about these cases.
Report any complications of pain or immediate bleeding, and describe the situation exactly, including the date, gestational age, health concerns, the way you did the inversion, whether it was your first attempt or not, and the time of complication. You can email me at gail@spinningbabies.com.