MYTH: Position changes can change the OP position in the labor
This hasn’t been studied like I’d like to it to be studied. The studies aren’t designed in a way that will answer anything, but regardless, 30 minutes of position changes are not enough to overcome the tension in the womb holding the baby in an unfavorable position.
These studies are why I developed the The Three Principles of Spinning Babies®.
First, you have to relax the involuntary muscles, and release tension or torsion in the muscle fibers and fascia making up the uterine ligaments. Second, you get gravity helping and third, move the pelvis in ways that open the level of the pelvis that the baby’s head is resting at.
If the head is stuck at the brim, you don’t open the bottom of the pelvis, for instance, and wonder why squatting works for some women and not for others. If your front doorbell rings, do you open the back door and wonder where your company is at?
Pelvic shape and size do have an effect on the course of posterior labor in a small percentage of women. A pelvic shape which is longer front to back allows a few women to have a posterior baby without back labor, as long as there isn’t another reason for backache, like a muscle spasm.
A pelvic shape which is triangularly (once called an android pelvis) can make it hard for a larger, posterior baby to fit through. A woman with a smaller than average android pelvis will need to, in my observations, eat carefully to get good protein and vegetables without a lot of sweets and white bread. Baby’s position is considered more important in the 2nd Trimester so baby can come into the brim months later from the left side, especially if in a first-birth or first vaginal birth. This may help avoid the scenario I have often seen of trying to help a large OP baby to turn around at 8 months to get settled into position for birth.
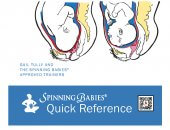
The baby’s back shifts right and left and right again, trying to turn his little forehead out of the narrow pointy space at the mother’s pubic bone. But the pelvis isn’t round so he can’t. He’ll have to come up and out, away from the brim to turn. He can only do that if the mom relaxes her ligaments, and gets upside down a bit each day.
It isn’t always comfortable, of course, to be 8 months pregnant and hang upside down for a minute. And even then, some of these moms need bodywork to overcome the muscle spasms in their round or broad ligaments. It’s much easier to do at 4 and 5 months pregnant. Even 6 months. If these few OP babies aren’t able to navigate their mother’s pelvic brim, they will have to be born by cesarean. The problem is that few people, and I mean providers, can tell who will be the one that gets stuck and who will be the one to get through.
Someone with a round pelvic brim has a much better chance of experiencing their posterior baby rotate in labor. Depending on various factors, like eating in labor, keeping hydrated, leaning forward, being patient, resting belly down (somewhat), avoiding positions on her back, having her water broke or an epidural that increases the likelihood of a challenge with the labor (length, vacuum or surgery), baby may come around readily or only eventually. A long labor can soften up tight spots on the route out.
The pelvic shape isn’t the only consideration, of course. The soft tissues are more often the case, especially when they aren’t soft at all!
Remember, a pelvis shape isn’t a pelvic type. Learn more about the racist roots of name calling the pelvis by typing the pelvic according to racial heritage. And at the same time, consider the personal environment of the baby you are caring for (as provider or parent) and their needs for engagement, rotation, and descent through the pelvis they get to be born through!
 There is a difference in
There is a difference in