The Difference a Sidelying Release Makes

Here is a labor attempting to begin. Contractions start but neither move labor along nor let the woman rest. Twice before this non-progressing latent labor ended in surgery. The role of this doula was to bring her positive attitude and practical strategies. Let’s gain understanding of which of the techniques may have actually advanced labor progress and which ones, though classic, may not have addressed the situation in play.
Of course, we are looking through the lens of Spinning Babies
We review the good decisions of this doula with a perspective still little known in the doula world.
Beatrice writes,
“Just to let you know I’ve just used your techniques today with amazing results! My lady was really hoping for a VBAC after two emergency c-sections, she went into labour yesterday but her contractions were really mild inconsistent and not getting her anywhere… so she went for a long walk in the park, up and down hills and after eating a nice meal, she went home to put her kids to bed and to rest for a little while.”
Here we see the classic, natural birth movement’s strategy to allow the simple passage of time to support the flow of labor. Allowing labor to establish on its own is a healthy and respectful choice…when such a strategy matches the labor situation.
In this case, the labor didn’t pick up and night turned to day. Beatrice also knew that this particular mom had a history of emergency cesareans.
An emergency cesarean is surgical birth after the onset of labor. Whether the mother or baby are in a life threatening situation or a long leisurely labor is not defined by this way of using the term “emergency.” In most cases, finishing the birth with an “emergency cesarean” isn’t an emergency at all. It’s only a few cesareans in which the baby or parent are in danger and need immediate life saving surgery to escape severe injury or death.
Most of the time, a lot of time passes as the birth team tries many strategies to help the baby down through the pelvis. After more time, the birth team (including the birthing member!) decides enough-is-enough and a cesarean is now the best option for a safe birth. In these situations, the contractions are strong enough to, but don’t:
- Rotate the baby
- Dilate the cervix, and
- Bring baby down the pelvis
For Beatrice’s “Lady”, these strong contractions weren’t able to accomplish these three important measures of labor progress. This is exactly the scenario we hope to avoid repeating when supporting a VBAC mother. VBAC is Vaginal Birth After a Cesarean (for a previous birth).

In most cases, emergency cesareans are not because the pelvis is too small, but rather the babies aren’t angled into their smallest diameters. Like a swimmer diving into the pool, a birthing baby “makes the smallest splash” (meaning the baby slips most easily into the world) when baby pulls the chin into the chest and brings the shoulders and arms close to the chest to make the body “smaller”.
Beatrice knew that baby could be helped into the pelvis. She wasn’t specific in her email where in the pelvis she believed baby to be. Remember, they hadn’t gotten to the hospital yet to have the nurse or provider check the birthing person’s cervix and check which level of the pelvis they found the baby at.
“We started a routine of stretching her psoas muscles followed by lunges and wide side squatting and calf stretches up and down the steps and the birthing ball…”
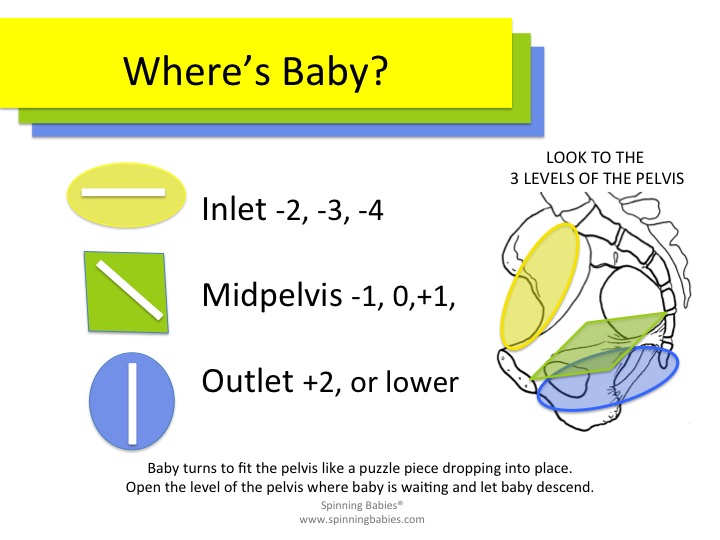
Let’s look at these techniques to see which part of the birth journey these techniques give specific help for making room for the baby. There are three levels to the pelvis, three gates, as it were for the baby to pass through.
The inlet (top entrance to the bony tunnel)
The Midpelvis (middle)
The Outlet (bottom, exit of the bony tunnel)
I suspect from the history of repeat cesareans followed by a vaginal birth that the missing factor for the earlier births was fetal engagement. It may be that in the earlier births, and for the long leisurely beginning of this labor, the babies were up at the entrance, the brim, or inlet to the pelvis. I may be wrong, but this is a common cause of “emergency cesarean” and the subsequence avoidance of such an “emergency” by helping baby engage.
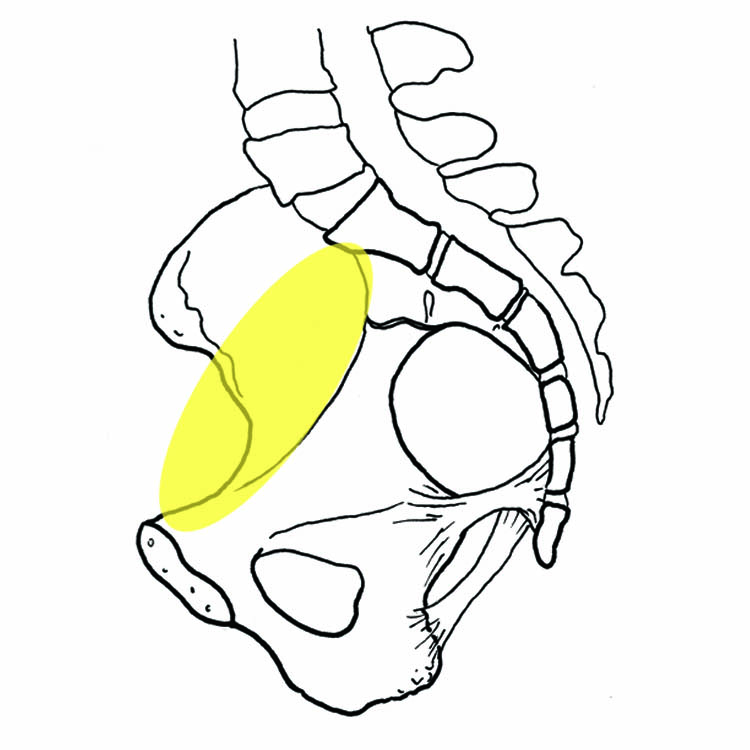
The inlet (top entrance to the bony tunnel) Stretching her psoas muscles, Forward Lunges are another way of helping the psoas muscle pair lengthen. There is a particular way of doing them that “wakens” the psoas. Going up and down the steps helps some babies drop into the pelvis but many times there are less tiring ways to do help baby engage.
The birthing ball can be a help when pumped up properly to let the hips be slightly higher than the knees. For engaging baby, usually what is needed for labor progress first, turn some happy music on and do hip circles and figure eights.
If a birthing mother belly dances those moves may be preferable… actually its not common for belly dancers to have a long labor, so this is a silly addition. About 30-40 minutes of dancing or using the birth ball like a “dancing seat” is usual.

The Midpelvis (middle) Side Lunges or those lunges that look like a sword player are specific to the mid pelvis or outlet. Lunging to the side would not likely help baby drop into the pelvis. Wide side squatting may mean the knees go out to the side. This may help the bottom of the pelvis open but will close the top and reduce the chance that baby will drop into the pelvis. If baby is already deep in the pelvis these may be useful. Squats reveal their usefulness in 3 to 6 contractions. If you aren’t seeing good progress after that, try them again when baby is lower (if needed).
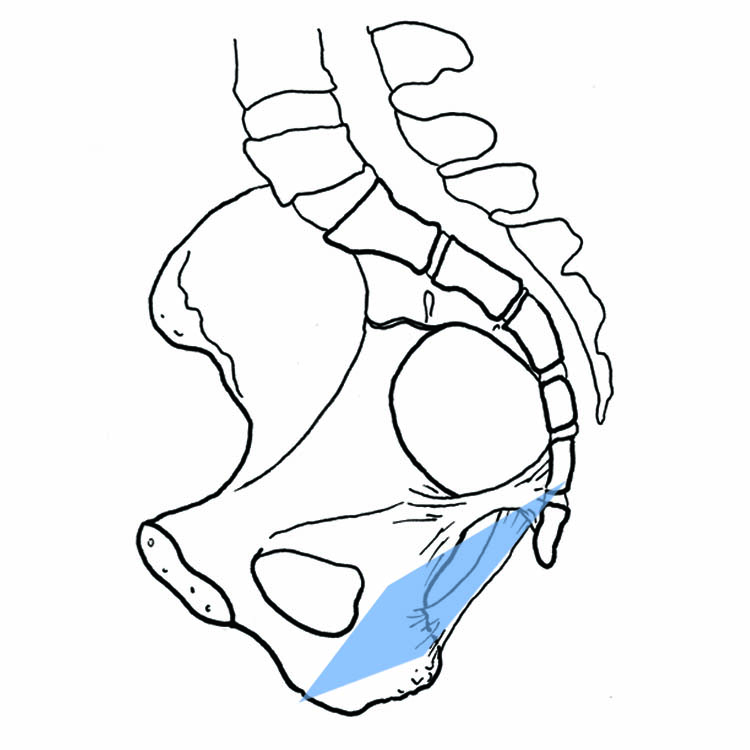
The Outlet (bottom, exit of the bony tunnel) Calf stretches can be helpful for the sacrum to move out of baby’s way. The mobile sacrum is dramatic for moving out of the way in the mid or lower pelvis, but may help fetal engagement at the top as well. I put it here because the effect of a calf stretch in labor might be minimal on pelvic mobility at the top of the pelvis but may be slightly better on the bottom. Daily calf stretches for a couple weeks followed by weeks of daily squatting would show the effectiveness of the calf stretch in the big picture, but an immediate effectiveness is less likely to occur.
The baby lines up with each of these openings in the pelvis by rotating. When the head lines up at each gate, the contractions can move the baby down. Balancing tight or loose muscles and untwisting any crooked ligaments help soften baby’s path through these three pelvic levels.
You may have noticed in the story that labor wasn’t active yet. Strong contractions are necessary. The womb has been working for many hours without building up a momentum necessary to move labor along.
The doula was thinking and the mother was now ready to try something new. They’d tried some gravity friendly positions and movement without success. Now they began the Queen of the Static Stretch techniques, the Sidelying Release. This is far more than lying on one’s side!
Done on both sides to relieve lopsided muscle tension in the pelvis, Sidelying Release is often the solution for uneven pelvic floor muscles. This baby didn’t seem to be so far down the pelvis to be on the pelvic floor yet. The doula is using Sidelying Release to help the mother get into active labor.
“…then Sidelying Release on both sides for the duration of three contractions. After nearly three hours of hard work she went in nice long bath… ” This description gives us the clue that Sidelying Release allowed a regular, strong labor pattern to establish over the next three hours. Then she took a gentle bath to adjust her mind to labor and perhaps find pain relief. When baby drops into the pelvis and comes on to the cervix for the first time, the emotional release as well as the added pressure deserves a little deep immersion in a warm (but not the exhausting heat of a hot tub) pool or bathtub. If a deep tub or shower isn’t available, a gentle version of shake-the-apple tree (jiggling the buttocks muscles) is another way to relax the pelvis.
2 hours later she was on her way to the hospital with contractions every five minutes, she was three cm on arrival [being 3 cm after 5 hours of stronger labor is a good indication that I was right with my assumption the baby was not engaged before the doulas good suggestions. Lack of engagement may have been the leading factor in the previous cesareans.] but continued mobilising [moving freely] until her contractions were much more intense and soon after she was feeling pressure with each contraction and we barely had time to reach the delivery suite for her to start pushing… baby was born soon after with a very smooth clean and gentle delivery no stitches… mother and baby went home a few hours later!”
Congratulations VBAC Family and Doula Beatrice! We, at Spinning Babies, are so happy to help!
And we appreciate the chance to discuss this lovely birth with you as an teaching tool for the 3 Levels Solutions.

You can learn more about 3 Levels Solutions to help you pick the right techniques sooner on the
Spinning Babies; Quick Reference Guide digital download for providers;
or
Spinning Babies; Parent Class for parents digital download.
US customers can visit the Spinning Babies online shop for the booklet or DVD.