Pelvimetry Can Still Be Worth Something
2011-02-15 |
Birth Anatomy

Pelvimetry has been abandoned by many as meaningless. It may not have importance to those who do not know what changes they might make in their practice protocols for variations in pelvi. For those who know that the pelvis is dynamic and changeable, there are women whose can adapt their birth preparation to their pelvic shape or variation. javascript:void(0)Achieving a dynamic balance is helpful for all women, enhancing labor ease and progress.”
The pelvic shape may be secondary to fetal rotation and flexion into the pelvis, but size and shape do take a role in childbirth. The fact that obstetric surgeons switch to cesarean surgery if the baby doesn’t fit doesn’t mean the rest of us are ignorant in ways to support the individual size and shape of the pelvis.
Though I’ve only been interested in a woman’s pelvic shape and size occasionally, not even annually when I was attending births regularly, there were situations when an interest was indicated.
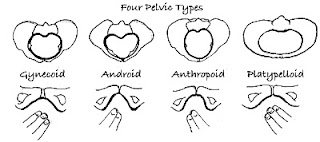
The woman with a gynecoid pelvis often finds that labor itself will eventually get the posterior baby rotated to any of the anterior positions, or in some cases, gives birth to a posterior baby.
In a woman with an android pelvis, if her baby at the end of pregnancy is rather large (for her) and in the posterior presentation, I note that the forehead can settle into the triangular shape of the anterior inlet making rotation next to impossible unless the round ligaments and broad ligaments can be loosened (first time mother issue and older mother typically) and the baby helped to reposition to the LOA then the baby may never engage, even with labor. We start with this mama in 2nd trimester to achieve a dynamic balance so that her baby comes into the brim in the LOA position.
The woman with an anthropoid pelvis will start labor with either an OA baby (if engaged) or a direct OP baby and in either case the baby may rotate on the pelvic floor or may be born without any need to rotate. Could these be the women with the 3-8 hour posterior labors that find that all the fuss wasn’t applicable to their experience?
In a woman with a platypelloid pelvis, her baby does need to get into the LOT position, usually with chin tucked in flexion, to enter the pelvis. Labor can be days shorter if this is achieved before labor rather than through long, hard, frequent contractions.
You see that the woman with the android pelvis, the fast sprinter or easy runner, may have an issue if her android pelvis runs on the small side and her baby is large (maybe she drinks more than a quart of milk daily and such foods that grow large babies). The woman with the platypelloid pelvis (only 5% of all) will be very interested in helping baby face her right hip (LOT or LOL in UK) to start labor. Overall, 65% of OP babies rotate to the OA by the end of labor. But starting labor in one of the anterior positions, or at least with a tucked chin, does make a difference for some pelvic types.
Most women can go into labor confidently without knowing whether their pelvis is round, oblong, or even triangular, but there are times when a little knowledge helps women prepare for labor and their providers pick techniques and exercises that promote rotation and descent rather than choosing common techniques at random, simply because they usually work and not knowing what the woman they sit with needs for this long labor.
Labor is worth it.
Come visit the blog. Spinning Babies Blog. www.spinningbabies.com